©2009-11 Alexandra's PHATE
Alexandra's P.H.A.T.E. © 2011 Alexandras P.H.A.T.E. All rights reserved. Reproduction of material from any pages without written permission is strictly prohibited.
Contact Us: 412.860.4557 | email
Content on this website is provided for informational purposes only and is not intended as a substitute for medical consultation. Please direct all inquires to your medical practitioner.
All StarBandKids and Orthomerica Images and information are Courtesy of Orthomerica Products, Inc. ©2011
Content on this website is provided for informational purposes only and is not intended as a substitute for medical consultation. Please direct all inquires to your medical practitioner.
All StarBandKids and Orthomerica Images and information are Courtesy of Orthomerica Products, Inc. ©2011
Logo artwork courtesy of Barry Linck. Visit his site at Phinmagic.com
Positional Plagiocephaly
Do you have questions about Plagiocephaly? What is it? How does it occur? Can it be corrected? Where do I go after diagnosis?
We have the answers to many of your Plagiocephaly questions, right here! If you happen to not find what you are looking for, please fill free to visit our "contact" page, and we will be happy to help any way that we can.
Follow Us!
What is Positional Plagiocephaly?
An infant’s skull is made up of free-floating bones that are separated by "sutures". The sutures allow the skull to mold for birthing and to expand with the growing brain.
While many infants are born with an abnormal head shape, most will correct themselves within six to eight weeks following the birth. When an abnormal head shape persists or isnt noticed (like in our personal case) it is important to determine the cause. A correct diagnosis is essential and should be made by a qualified specialist or nerosurgeon.
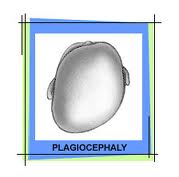
The most common Positional Head Deformity is Positional Plagiocephaly. Positional Plagiocephaly is caused when repeated external pressure is applied to one side of the back of the head and a flat spot occurs. The side of the head that is flattened will often be accompanied by a prominent forehead. It is also common for an infant with Positional Plagiocephaly to have misaligned ears (the ear on the effected side may be pulled forward and down and be larger then the unaffected ear) and facial asymmetry, with the affected side of the face having a fuller cheek, and a more prominent appearance. Facial asymmetry on the affected side can also include a jawbone that is tilted, and an eye that appears displaced and mismatched in size.
While many infants are born with an abnormal head shape, most will correct themselves within six to eight weeks following the birth. When an abnormal head shape persists or isnt noticed (like in our personal case) it is important to determine the cause. A correct diagnosis is essential and should be made by a qualified specialist or nerosurgeon.
The most common Positional Head Deformity is Positional Plagiocephaly. Positional Plagiocephaly is caused when repeated external pressure is applied to one side of the back of the head and a flat spot occurs. The side of the head that is flattened will often be accompanied by a prominent forehead. It is also common for an infant with Positional Plagiocephaly to have misaligned ears (the ear on the effected side may be pulled forward and down and be larger then the unaffected ear) and facial asymmetry, with the affected side of the face having a fuller cheek, and a more prominent appearance. Facial asymmetry on the affected side can also include a jawbone that is tilted, and an eye that appears displaced and mismatched in size.
Why is the term "positional" used?
The term Positional is used to differentiate from true Synostosis, which is a premature fusion of one or more of the skull sutures (Craniosynostosis) and requires surgery to repair. When the term Positional is used, it means that there is NO premature suture fusion and that an external pressure on the skull caused the deformity.
How Do I see Facial Asymmetry?
What is Facial Asymmetry?
Positional Plagiocephaly is not the only Positional Head Deformity, though it is by far the most common.
Positional Brachycephaly is when the entire back of the head is flat and the head has the appearance of being wide and short. Positional Brachycephaly is most often seen when a child sleeps entirely on the back of his head.
Positional Scaphocephaly is when the head is long and narrow. Positional Scaphocephaly can result when the infant is in a breech position during the pregnancy and the head becomes wedged underneath the mother’s ribs. Prematurity can also be a contributing factor to Positional Scaphocephaly.
Positional Brachycephaly is when the entire back of the head is flat and the head has the appearance of being wide and short. Positional Brachycephaly is most often seen when a child sleeps entirely on the back of his head.
Positional Scaphocephaly is when the head is long and narrow. Positional Scaphocephaly can result when the infant is in a breech position during the pregnancy and the head becomes wedged underneath the mother’s ribs. Prematurity can also be a contributing factor to Positional Scaphocephaly.



Is Positional Plagiocephaly the only positional head deformity?
Is Positional Plagiocephaly Just Cosmetic?
The external forces that push and mold the skull can also affect the features of the face causing facial asymmetry. Facial asymmetry is when one side of the face does not match up with the other side of the face. Most often the affected side will have a more pronounced forehead and possibly a cheek that is fuller then the other cheek. It is also possible to see the eye on the affected side appear displaced and mismatched in size and for the jaw to appear tilted. All or some of these factors can make the face appear lopsided.
It can be very difficult to see facial asymmetry. Most often parents have the feeling that something just does not look right. If you cannot readily see facial asymmetry place your baby in front of a mirror and look at your baby’s reflection. Facial asymmetry becomes very apparent using this method because the mirror will help show the baby’s face in a two dimensional plane.
It was believed that Positional Plagiocephaly was only a cosmetic disorder because it does not restrict brain growth or cause brain damage. However, there is now increasing evidence that other problems can arise, especially when facial asymmetry is present.
Some of the problems that can be experienced due to facial abnormalities include, problems with chewing and eating. Difficulty with vision could also become an issue and require corrective surgery to repair. While head shape abnormalities can possibly cause temporormandibular joint syndrome (The temporormandibular joint or TMJ is the joint that operates the jaw)
Furthermore, the American Medical Association defines that a cosmetic procedure changes normal structure of the body in order to improve appearance. While a reconstructive procedure is performed on an abnormal structure of the body to improve function, or return it to normal.
· Also of concern
The possibility of psychological disturbances due to an abnormal appearance also weighs heavily on parents’ minds. Knowing how conscientious children can be of their appearance, especially during the teenage years, is cause for concern for many parents that have an infant with Positional Plagiocephaly.
Some of the problems that can be experienced due to facial abnormalities include, problems with chewing and eating. Difficulty with vision could also become an issue and require corrective surgery to repair. While head shape abnormalities can possibly cause temporormandibular joint syndrome (The temporormandibular joint or TMJ is the joint that operates the jaw)
Furthermore, the American Medical Association defines that a cosmetic procedure changes normal structure of the body in order to improve appearance. While a reconstructive procedure is performed on an abnormal structure of the body to improve function, or return it to normal.
· Also of concern
The possibility of psychological disturbances due to an abnormal appearance also weighs heavily on parents’ minds. Knowing how conscientious children can be of their appearance, especially during the teenage years, is cause for concern for many parents that have an infant with Positional Plagiocephaly.
Who Do I see to diagnose Positional Plagiocephaly?
In the majority of cases, concern of Positional Plagiocephaly is first brought up to the child’s Pediatrician. While it is not unusual for a Pediatrician to refer a child to a Pediatric Neurologist, a Pediatric Neurosurgeon, or a Pediatric Craniofacial Plastic Surgeon, it is becoming more common for a Pediatrician alone to make the diagnosis, and suggest treatments. However, it is essential to deal with a knowledgeable physician to obtain a proper diagnosis. If there is any doubt on the part of the parents then seek another professional opinion, preferably with a doctor experienced with Positional Plagiocephaly.
What Kind of tests will be run?
The most common tests performed are X-Rays, CT-Scans and MRI’s. Though in most cases only one diagnostic test will be performed, it is possible to have a combination of just two or of all three tests. Testing is typically done to confirm that the head deformity is not being caused by a true Synostosis (a premature fusion of one or more skull sutures). However, increasing evidence suggests that Positional Plagiocephaly differs from Craniosynostosis Plagiocephaly in outward appearance. This finding is leading more doctors who are well versed in Positional Plagiocephaly to feel confident in making a diagnosis without additional testing. But again, it is important for the parents to feel confident with the doctor and seek other opinions if there is doubt or uncertainty.
What Causes Positional Plagiocephaly?
There are several possible causes of Positional Plagiocephaly. The most common causes are:
· In Utero Constraint
When a baby develops in a womb that is constricted it can lead to Positional Plagiocephaly. Constriction of the womb can be caused by a variety of factors including, a multiple pregnancy with two or more fetuses, a small or malformed uterus, a small maternal pelvis, or an inappropriate amount of amniotic fluid. A baby that is in a breech position can also develop Positional Plagiocephaly if the baby’s head becomes wedged under the mother’s ribs.
· Prematurity
The skull of a premature infant can be very soft and malleable making the head more susceptible to remolding due to external pressures.
· Back Sleeping
In 1992 the American Academy of Pediatrics’ (AAP) made the recommendation that infants should sleep on their backs to reduce the risk of SIDS (Sudden Infant Death Syndrome), which launched the “Back To Sleep Campaign”. While the Back to Sleep Campaign has made tremendous strides in reducing SIDS, there has also been a dramatic increase of the number of infants suffering from Positional Plagiocephaly due to back sleeping. Parents were not given enough information regarding back sleeping and how the infant’s sleeping position should be alternated to prevent constant sleeping on the same side, nor were parents informed of the importance of “tummy time” during play. Consequently, because of the fear that many parents have regarding SIDS, many infants spend almost 100% of their time on their backs. Between infant car seats, infant carriers, bouncy seats, infant swings and sleeping on a mattress at night an infant spends little or no time without external pressure applied to the back of the head which leads to a high susceptibility to Positional Plagiocephaly.
· Congenital Muscular Torticollis
Congenital Muscular Torticollis (CMT), also known as Twisted Neck or Wry Neck, is a condition that is usually caused when one or more of the neck muscles is shortened or tightened on one side of the neck. This causes the baby’s head to tilt and/or to turn in one particular direction. CMT can be very blatant or very subtle. Parents are usually the first to notice the more subtle cases. If your baby tends to always look in one direction then it is very possible that CMT could be the cause. If you suspect that your child may have CMT it is important to have it diagnosed by a physician and to have it treated.
Treatment of CMT usually consists of physical therapy to lengthen and loosen the affected muscle(s). Only in VERY severe cases is surgery needed to repair the muscle(s).
For more information on CMT please click here.
· In Utero Constraint
When a baby develops in a womb that is constricted it can lead to Positional Plagiocephaly. Constriction of the womb can be caused by a variety of factors including, a multiple pregnancy with two or more fetuses, a small or malformed uterus, a small maternal pelvis, or an inappropriate amount of amniotic fluid. A baby that is in a breech position can also develop Positional Plagiocephaly if the baby’s head becomes wedged under the mother’s ribs.
· Prematurity
The skull of a premature infant can be very soft and malleable making the head more susceptible to remolding due to external pressures.
· Back Sleeping
In 1992 the American Academy of Pediatrics’ (AAP) made the recommendation that infants should sleep on their backs to reduce the risk of SIDS (Sudden Infant Death Syndrome), which launched the “Back To Sleep Campaign”. While the Back to Sleep Campaign has made tremendous strides in reducing SIDS, there has also been a dramatic increase of the number of infants suffering from Positional Plagiocephaly due to back sleeping. Parents were not given enough information regarding back sleeping and how the infant’s sleeping position should be alternated to prevent constant sleeping on the same side, nor were parents informed of the importance of “tummy time” during play. Consequently, because of the fear that many parents have regarding SIDS, many infants spend almost 100% of their time on their backs. Between infant car seats, infant carriers, bouncy seats, infant swings and sleeping on a mattress at night an infant spends little or no time without external pressure applied to the back of the head which leads to a high susceptibility to Positional Plagiocephaly.
· Congenital Muscular Torticollis
Congenital Muscular Torticollis (CMT), also known as Twisted Neck or Wry Neck, is a condition that is usually caused when one or more of the neck muscles is shortened or tightened on one side of the neck. This causes the baby’s head to tilt and/or to turn in one particular direction. CMT can be very blatant or very subtle. Parents are usually the first to notice the more subtle cases. If your baby tends to always look in one direction then it is very possible that CMT could be the cause. If you suspect that your child may have CMT it is important to have it diagnosed by a physician and to have it treated.
Treatment of CMT usually consists of physical therapy to lengthen and loosen the affected muscle(s). Only in VERY severe cases is surgery needed to repair the muscle(s).
For more information on CMT please click here.
What Treatments are available for Positional Plagiocephaly?
Before discussing treatment methods, the factor that age plays in treatment must be explained. In all cases of treatment, aside from surgery, you are capturing the rapid growth of the child's skull and redirecting it to achieve symmetry. Since the vast majority of cranial growth (approximately 80%) is achieved in the first 12 months of life the greatest amount of correction will be achieved during this time. Although many children do receive good results with cranial orthosis in the second year of life, the length of treatment is longer and the correction may not be as great. For this reason it is imperative for parents to seek medical attention as soon as possible, deal with a physician that is knowledgeable in Positional Plagiocephaly, and choose a treatment course that they are confident with.
Positional Plagiocephaly is currently subject to a huge debate over its treatments. In the past, surgery was routinely performed, more than likely as a misdiagnosis for a true Synostosis. Though in extremely severe cases of Positional Plagiocephaly, surgery may still be suggested. If the child is young enough to undergo another form of treatment, it is no longer the norm and a second opinion should be sought.
Currently the most common forms of treatment are reposition therapy and helmet or band therapy. Some doctors argue that Positional Plagiocephaly will correct on it’s own as the child grows and becomes developmentally mature, resulting in less time spent on the back. This can be true in mild cases, but most parents that have children with moderate or severe cases are not willing to take that gamble and opt for treatment. Before a treatment is decided upon it is best to consider all of the factors. It is commonly believed that aggressive reposition therapy is best utilized when a child is between the ages of 0-6 months depending on severity of the Positional Plagiocephaly. After six months (or sooner depending on the child), it is much harder to control the side that the baby sleeps on so reposition therapy may not be as affective. Helmet or band therapy is also best started at an early age, usually around 5 months. Though some bands and helmets can be used as late as 18 months, effectiveness is greater when the baby is younger. Because of this, parents along with doctors should make educated decisions based on the individual baby, the baby’s age and the degree of Positional Plagiocephaly and facial asymmetry.
What is Repositioning Therapy? (Click for Repositioning Techniques)
Reposition therapy is simply the concept of repositioning the baby so that he does not rest on the flat spot. It is believed that by removing the external pressure, the flat area will “round out” as the head grows.
Before trying reposition therapy it is important that the baby be cleared of Torticollis. If the baby has Torticollis it is important that parents discuss this with the baby’s physician and utilize physical therapy to stretch the neck muscles.
If reposition therapy is to be used, the baby’s physician should be consulted on the best way to achieve this. Some common practices of reposition therapy are placing a rolled up towel or blanket beneath the back of the flattened side to prevent the baby from rolling onto the affected side. Another common tactic is placing crib toys on the opposite side of the flattening to make the child look in that direction. Adding supervised "Tummy Time" while the child is awake and playing, is another important part of repositioning. Adding supervised "Tummy Time" while the child is awake and playing, is another important part of repositioning.
When tummy time is first introduced to a baby, it is best done is short intervals of only about a minute or two at a time. As the baby gains muscle control and begins to enjoy tummy time, the intervals can be increased. This not only has the benefit of allowing an infant to strengthen many muscles that are not used when laying on the back, but it also allows the back of the head to have some time without external pressure pushing up against it.
There are several different methods that can be used for reposition therapy. A little bit of creativity is also of great benefit in this area. However, always keep safety in mind and never place an item in the crib that could be harmful.
Before trying reposition therapy it is important that the baby be cleared of Torticollis. If the baby has Torticollis it is important that parents discuss this with the baby’s physician and utilize physical therapy to stretch the neck muscles.
If reposition therapy is to be used, the baby’s physician should be consulted on the best way to achieve this. Some common practices of reposition therapy are placing a rolled up towel or blanket beneath the back of the flattened side to prevent the baby from rolling onto the affected side. Another common tactic is placing crib toys on the opposite side of the flattening to make the child look in that direction. Adding supervised "Tummy Time" while the child is awake and playing, is another important part of repositioning. Adding supervised "Tummy Time" while the child is awake and playing, is another important part of repositioning.
When tummy time is first introduced to a baby, it is best done is short intervals of only about a minute or two at a time. As the baby gains muscle control and begins to enjoy tummy time, the intervals can be increased. This not only has the benefit of allowing an infant to strengthen many muscles that are not used when laying on the back, but it also allows the back of the head to have some time without external pressure pushing up against it.
There are several different methods that can be used for reposition therapy. A little bit of creativity is also of great benefit in this area. However, always keep safety in mind and never place an item in the crib that could be harmful.
What are corrective helmets and bands?
The first corrective device offered for Positional Plagiocephaly was the Molding Helmet. The original molding helmet introduced in 1979 was designed with the basic concept that if you surround the asymmetrical infant head with a symmetrical (normal) mold, the skull will grow into the mold and take on the shape of the mold resulting in a normal shaped head. An alternative technique, Dynamic Orthotic CranioplastySM was subsequently developed as a more proactive approach to treatment of Positional Plagiocephaly. In this technique, the device was specifically designed to apply gentle pressure to the area of the head where growth was not wanted, while leaving space where growth was needed. With this technique, the child is seen on a weekly to biweekly basis to have adjustments made to the band to ensure proper growth of the head and optimum correction of the deformity. Today we are seeing a large variety of bands and helmets, many of which take into consideration the concepts of the original molding helmets and the DOC Band®. The child’s physician will be able to direct parents on where to obtain a helmet or band. It is important that parents research the success rate of any helmet or band under consideration. If a particular helmet or band does not have a good success rate then another should be found.
Bands and Helmets come in several different designs but two things that they all have in common is that they are all light-weight and they are all custom made to fit the individual baby’s head. In order for the band or helmet to be custom fit there must be a casting done of the child’s head.
The length of treatment time for a helmet or band is dependent on several things. The age at which the baby starts the therapy, the particular design of the band or helmet used, the rate at which the individual baby grows, and the degree of Positional Plagiocephaly all play factors into determining the length of treatment necessary. Therefore, it cannot be stated how long therapy will last for an individual baby. However, on average most children will complete therapy within 2- 6 months, but again this is only an average and it is possible for an individual baby to complete therapy earlier or later depending on the factors listed above.
Bands and Helmets come in several different designs but two things that they all have in common is that they are all light-weight and they are all custom made to fit the individual baby’s head. In order for the band or helmet to be custom fit there must be a casting done of the child’s head.
The length of treatment time for a helmet or band is dependent on several things. The age at which the baby starts the therapy, the particular design of the band or helmet used, the rate at which the individual baby grows, and the degree of Positional Plagiocephaly all play factors into determining the length of treatment necessary. Therefore, it cannot be stated how long therapy will last for an individual baby. However, on average most children will complete therapy within 2- 6 months, but again this is only an average and it is possible for an individual baby to complete therapy earlier or later depending on the factors listed above.

